Fill Out a Valid Tennessee First Report Form
In the realm of workplace safety and compliance, the Tennessee Department of Labor and Workforce Development mandates the use of the Employer’s First Report of Work Injury or Illness form, a crucial document that serves as the primary mechanism for reporting any workplace injury or illness. This requirement, grounded in the Tennessee Workers' Compensation Law, underscores the state’s commitment to maintaining a safe and healthy work environment, ensuring timely and accurate reporting of workplace incidents. Through this form, employers are obliged to detail the nature, cause, and extent of the injury or illness, providing a comprehensive account that includes the employee’s personal details, employment status, and the specifics of the incident, such as the date, time, and how the injury or illness occurred. The legal framework also emphasizes the seriousness of furnishing false, incomplete, or misleading information, categorizing such actions as criminal offenses punishable by imprisonment, fines, and denial of insurance benefits. Moreover, the state facilitates support for stakeholders through a Benefit Review System, offering guidance and assistance from workers' compensation specialists. This robust process underscores Tennessee’s proactive approach to workers' compensation, aiming not only to protect employees but also to provide a structured pathway for reporting, investigation, and resolution of work-related injuries or illnesses.
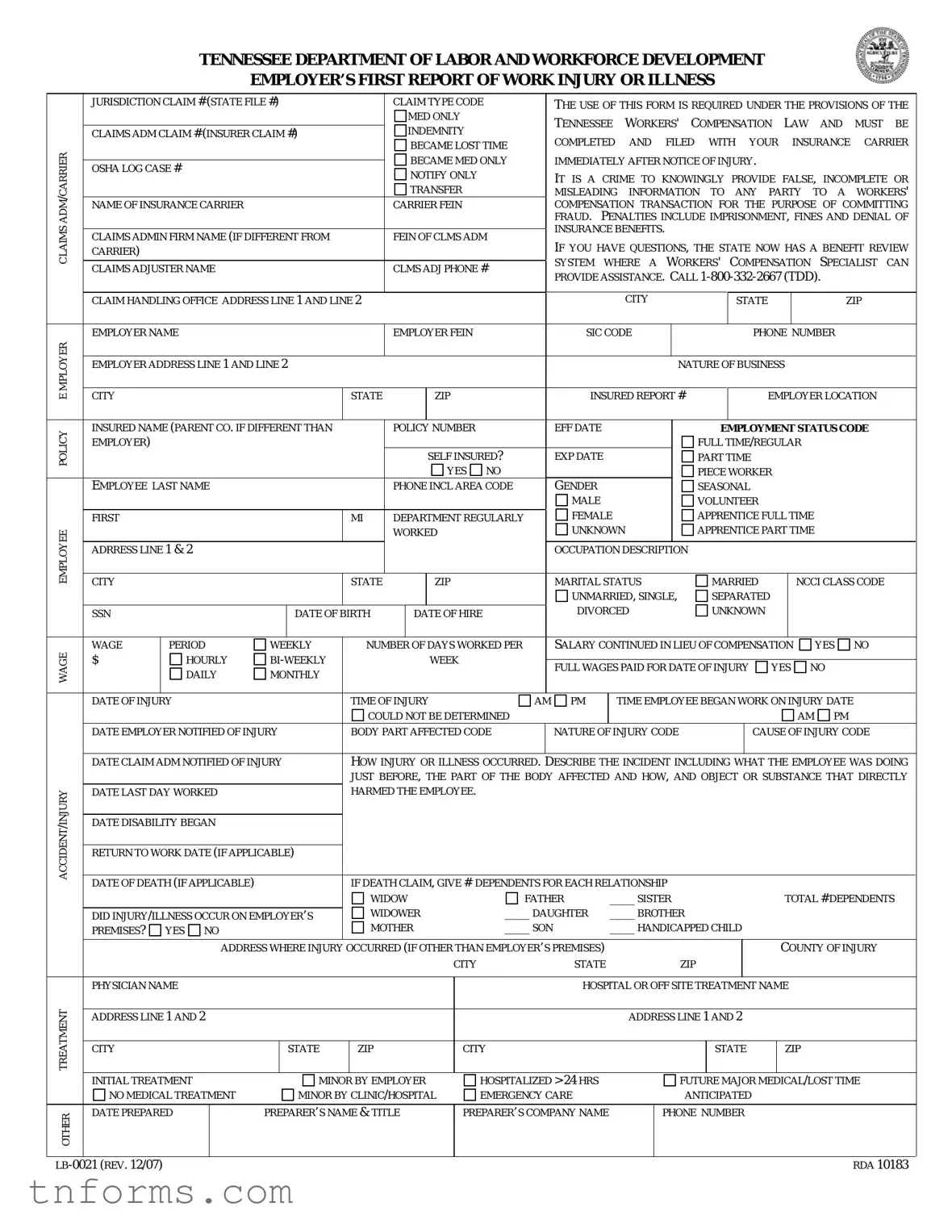
Example - Tennessee First Report Form
TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT
EMPLOYER’S FIRST REPORT OF WORK INJURY OR ILLNESS
|
JURISDICTION CLAIM # (STATE FILE #) |
|
|
|
CLAIM TYPE CODE |
|
THE USE OF THIS FORM IS REQUIRED UNDER THE PROVISIONS OF THE |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
MED ONLY |
|
|
TENNESSEE |
WORKERS' |
|
COMPENSATION |
LAW |
AND |
MUST |
BE |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
INDEMNITY |
|
|
|
|||||||||||||||||||||
|
CLAIMS ADM CLAIM # (INSURER CLAIM #) |
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
COMPLETED |
AND |
FILED WITH |
YOUR |
|
|
INSURANCE |
CARRIER |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
BECAME LOST TIME |
|
|
|
|||||||||||||||||||||
CARRIER |
|
|
|
|
|
|
|
|
|
|
|
|
IT IS A CRIME TO KNOWINGLY PROVIDE FALSE, INCOMPLETE OR |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
TRANSFER |
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
BECAME MED ONLY |
|
IMMEDIATELY AFTER NOTICE OF INJURY. |
|
|
|
|
|
|
||||||||||||||||
|
OSHA LOG CASE # |
|
|
|
|
|
|
|
NOTIFY ONLY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MISLEADING INFORMATION TO ANY PARTY TO A WORKERS' |
|||||||||||||||||||
ADM |
NAME OF INSURANCE CARRIER |
|
|
|
|
|
|
CARRIER FEIN |
|
|
COMPENSATION TRANSACTION FOR THE PURPOSE OF COMMITTING |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FRAUD. |
PENALTIES INCLUDE IMPRISONMENT, FINES AND DENIAL OF |
|||||||||||||||||||
CLAIMS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INSURANCE BENEFITS. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
CLAIMS ADMIN FIRM NAME (IF DIFFERENT FROM |
|
|
|
FEIN OF CLMS ADM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
IF YOU HAVE QUESTIONS, THE STATE NOW HAS A BENEFIT REVIEW |
||||||||||||||||||||||||||||||||
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
CARRIER) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SYSTEM |
WHERE A |
WORKERS' COMPENSATION |
SPECIALIST |
CAN |
|||||||||||||||
|
CLAIMS ADJUSTER NAME |
|
|
|
|
|
|
CLMS ADJ PHONE # |
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
PROVIDE ASSISTANCE. CALL |
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
CLAIM HANDLING OFFICE ADDRESS LINE 1 AND LINE 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
|
ZIP |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
EMPLOYER NAME |
|
|
|
|
|
|
EMPLOYER FEIN |
|
|
SIC CODE |
|
|
|
|
|
|
|
PHONE NUMBER |
|
|
|||||||||||||||
MPLOYERE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
CITY |
|
|
|
|
|
|
STATE |
ZIP |
|
|
INSURED REPORT # |
EMPLOYER LOCATION |
|
|||||||||||||||||||||||
|
EMPLOYER ADDRESS LINE 1 AND LINE 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NATURE OF BUSINESS |
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
POLICY |
INSURED NAME (PARENT CO. IF DIFFERENT THAN |
|
|
|
POLICY NUMBER |
|
EFF DATE |
|
|
|
|
|
|
EMPLOYMENT STATUS CODE |
|
|||||||||||||||||||||
EMPLOYER) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FULL TIME/REGULAR |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
SELF INSURED? |
|
EXP DATE |
|
|
|
|
|
PART TIME |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
|
GENDER |
|
|
|
|
|
|
|
PIECE WORKER |
|
|
|
|
|
|
||||||
|
EMPLOYEE LAST NAME |
|
|
|
|
|
|
PHONE INCL AREA CODE |
|
|
|
|
|
|
|
|
SEASONAL |
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MALE |
|
|
|
|
|
|
|
VOLUNTEER |
|
|
|
|
|
|
|||||
|
FIRST |
|
|
|
|
|
|
MI |
|
DEPARTMENT REGULARLY |
|
FEMALE |
|
|
|
|
|
APPRENTICE FULL TIME |
|
|
|
|||||||||||||||
EMPLOYEE |
|
|
|
|
|
|
|
|
|
|
WORKED |
|
|
UNKNOWN |
|
|
|
APPRENTICE PART TIME |
|
|
|
|||||||||||||||
ADRRESS LINE 1 & 2 |
|
|
|
|
|
|
|
|
|
|
|
|
OCCUPATION DESCRIPTION |
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
CITY |
|
|
|
|
|
|
STATE |
ZIP |
|
|
MARITAL STATUS |
|
|
|
|
MARRIED |
|
|
NCCI CLASS CODE |
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
UNMARRIED, SINGLE, |
|
|
SEPARATED |
|
|
|
|
|
|
||||||||||
|
SSN |
|
|
|
|
DATE OF BIRTH |
|
|
DATE OF HIRE |
|
DIVORCED |
|
|
|
|
UNKNOWN |
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
WAGE |
WAGE |
|
PERIOD |
WEEKLY |
|
NUMBER OF DAYS WORKED PER |
|
SALARY CONTINUED IN LIEU OF COMPENSATION |
|
YES |
NO |
|
||||||||||||||||||||||||
$ |
|
HOURLY |
|
|
|
|
|
WEEK |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
FULL WAGES PAID FOR DATE OF INJURY |
YES NO |
|
|
||||||||||||||||||||||||
|
|
|
DAILY |
MONTHLY |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
DATE OF INJURY |
|
|
|
|
TIME OF INJURY |
|
AM PM |
|
|
TIME EMPLOYEE BEGAN WORK ON INJURY DATE |
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
COULD NOT BE DETERMINED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AM |
PM |
|
|
||||||
|
DATE EMPLOYER NOTIFIED OF INJURY |
|
BODY PART AFFECTED CODE |
|
NATURE OF INJURY CODE |
|
|
|
|
|
CAUSE OF INJURY CODE |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
DATE CLAIM ADM NOTIFIED OF INJURY |
|
HOW INJURY OR ILLNESS OCCURRED. |
DESCRIBE THE INCIDENT INCLUDING WHAT THE EMPLOYEE WAS DOING |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
JUST BEFORE, THE PART OF THE BODY AFFECTED AND HOW, AND OBJECT OR SUBSTANCE THAT DIRECTLY |
|||||||||||||||||||||||||||
INJURY |
DATE LAST DAY WORKED |
|
|
|
|
HARMED THE EMPLOYEE. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE DISABILITY BEGAN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
ACCIDENT/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RETURN TO WORK DATE (IF APPLICABLE) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
IF DEATH CLAIM, GIVE # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
DATE OF DEATH (IF APPLICABLE) |
|
|
|
DEPENDENTS FOR EACH RELATIONSHIP |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
WIDOW |
|
|
|
FATHER |
|
____ SISTER |
|
|
|
|
|
|
|
TOTAL # DEPENDENTS |
||||||||||||
|
|
|
|
|
|
WIDOWER |
|
|
____ DAUGHTER |
|
____ BROTHER |
|
|
|
|
|
|
|
|
|||||||||||||||||
|
DID INJURY/ILLNESS OCCUR ON EMPLOYER’S |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
PREMISES? |
YES NO |
|
|
|
|
|
MOTHER |
|
|
____ SON |
|
____ HANDICAPPED CHILD |
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
ADDRESS WHERE INJURY |
OCCURRED (IF OTHER THAN EMPLOYER’S PREMISES) |
|
|
|
|
|
|
|
|
|
|
|
COUNTY OF INJURY |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
|
|
|
|
ZIP |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
PHYSICIAN NAME |
|
|
|
|
|
|
|
|
|
|
|
|
HOSPITAL OR OFF SITE TREATMENT NAME |
|
|
|
|||||||||||||||||||
TREATMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS LINE 1 AND 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS LINE 1 AND 2 |
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
CITY |
|
|
|
|
STATE |
|
ZIP |
|
CITY |
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
ZIP |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
INITIAL TREATMENT |
|
|
MINOR BY EMPLOYER |
|
|
HOSPITALIZED > 24 HRS |
|
|
|
|
|
|
FUTURE MAJOR MEDICAL/LOST TIME |
|
|||||||||||||||||||||
|
NO MEDICAL TREATMENT |
|
|
MINOR BY CLINIC/HOSPITAL |
EMERGENCY CARE |
|
|
|
|
|
|
ANTICIPATED |
|
|
|
|
|
|
||||||||||||||||||
OTHER |
DATE PREPARED |
|
PREPARER’S NAME & TITLE |
|
PREPARER’S COMPANY NAME |
|
|
PHONE NUMBER |
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RDA 10183 |
||||
Form Breakdown
| Fact Name | Description |
|---|---|
| Governing Law | The form is required under the provisions of the Tennessee Workers' Compensation Law. |
| Usage Requirement | Employer’s First Report of Work Injury or Illness must be completed and filed with the insurance carrier immediately after notice of an injury. |
| Fraud Warning | It is a crime to knowingly provide false, incomplete, or misleading information for the purpose of committing fraud. Penalties include imprisonment, fines, and denial of insurance benefits. |
| Assistance Available | The State offers a Benefit Review System where a workers' compensation specialist can provide assistance. A contact number is provided for inquiries (1-800-332-2667). |
| Insurance Carrier Information | Details of the insurance carrier, including the name, FEIN, and claims adjuster information, are required on the form. |
| Employer Information | The form requires comprehensive information about the employer, including name, FEIN, and the specific location where the injury occurred. |
| Employee Information | Information about the injured or ill employee, including name, gender, employment status, and details of the injury or illness, must be reported. |
| Treatment and Injury Details | Details on the nature of the injury or illness, how and where the injury occurred, initial treatment provided, and if the injury/illness occurred on the employer’s premises are to be included. |
Detailed Instructions for Filling Out Tennessee First Report
When an employee experiences a work-related injury or illness, completing the Tennessee First Report form is a crucial step in the process. This form ensures that the details of the incident are officially recorded and helps in facilitating the workers' compensation process. Below are the step-by-step instructions for completing the form.
- Jurisdiction Claim # (State File #): Enter the claim number assigned by the state jurisdiction.
- Claim Type Code: Indicate whether it is a MED ONLY or INDEMNITY CLAIM.
- ADM Claim # (Insurer Claim #): Provide the claim number given by the insurance carrier.
- Carrier, FEIN: Enter the name and Federal Employer Identification Number of the insurance carrier.
- Claims Admin Firm Name: If different, write the name and FEIN of the claims administration firm.
- Claims Adjuster Name, Phone #: Fill in the adjuster's information who is handling the claim.
- Employer Information: Include the employer's name, FEIN, SIC code, phone number, city, state, zip, location, and address.
- Policy Information: Insert the policy number, effective and expiration dates, and confirm if self-insured.
- Employee Information: Enter the employee's details including last name, gender, marital status, address, phone number, occupation, NCCI class code, SSN, date of birth, and date of hire.
- Employment Status Code: Specify the employment status such as full-time, part-time, seasonal, etc.
- Incident Information: Document the date of injury, time of injury, how and where the injury occurred, body part affected, nature and cause of the injury, and if it happened on the employer's premises.
- Wage Information: Fill in the wage, wage period, number of days worked per week, and indicate if full wages were paid for the date of injury.
- Medical Information: Provide details of the initial treatment and if future major medical/lost time is anticipated.
- Additional Details: If applicable, include information about any death benefits, dependents, and the treatment provider.
- Preparer’s Information: Include the name, title, company name, and phone number of the person preparing the form.
Once the form is filled out, it should be reviewed for accuracy before submitting it to the insurance carrier. This submission is a critical step in ensuring the injured worker receives the appropriate medical care and benefits in a timely manner. The information provided also aids the insurance carrier in investigating and managing the claim effectively.
More About Tennessee First Report
What is the purpose of the Employer’s First Report of Work Injury or Illness in Tennessee?
This form serves as a mandatory document under the Tennessee Workers' Compensation Law for employers to report any work-related injury or illness. It must be completed and forwarded to the insurance carrier immediately after the employer is notified of an injury or illness. Its main purpose is to ensure that all relevant information regarding the incident is officially recorded and reported to the designated insurance carrier, facilitating the process of claims management and benefits distribution under the provisions of the law.
Who is responsible for submitting this form?
The employer is responsible for completing and submitting the Employer’s First Report of Work Injury or Illness. This duty falls upon the employer immediately after they are notified of an employee's work-related injury or illness. It is crucial for employers to gather all necessary information and report it accurately to their insurance carrier to comply with Tennessee's Workers' Compensation Law and ensure the proper handling of the worker’s compensation claim.
Are there penalties for providing false information on this form?
Yes, it is considered a criminal offense to knowingly provide false, incomplete, or misleading information on the Employer’s First Report of Work Injury or Illness. Such actions are undertaken with the intent to commit fraud against the workers' compensation system. Individuals found guilty of this offense may face serious consequences, including imprisonment, fines, and the denial of claims insurance benefits. It underscores the importance of providing accurate and complete information when filling out the form.
What should be done if there is anticipation of future medical treatment or lost time due to the injury?
If there is an expectation of significant medical treatment or lost time from work due to the injury, the employer must indicate this on the form. Specifically, the section titled "Initial Treatment" requires a selection that best describes the anticipated level of medical intervention or absence from work. Choices include options for no medical treatment, treatment by a minor clinic/hospital, emergency care, hospitalization for more than 24 hours, and other. Anticipating future medical or lost time needs helps the insurance carrier understand the potential complexity and severity of the claim, thereby allowing for more effective management of the injury or illness case.
Common mistakes
Filling out the Tennessee Department of Labor and Workforce Development Employer's First Report of Work Injury or Illness form is a crucial step in beginning the workers' compensation claim process. However, mistakes can disrupt or delay benefits for the injured worker. Here are ten common missteps to avoid:
- Incorrect or incomplete information: It's essential to provide accurate details throughout the form. Submitting incorrect data or leaving sections blank can lead to delays in processing the claim.
- Failing to list the precise time of injury: The exact time when the injury occurred needs to be documented. Approximations can cause issues in verifying the claim.
- Not detailing the injury accurately: The section asking for a description of the injury or illness, including how it happened, requires a comprehensive explanation. Vague descriptions may not suffice.
- Overlooking the importance of the date employer was notified: This date is crucial as it affects deadlines for both employers and insurance carriers to take action on a claim.
- Incorrect classification of employment status: Accurately indicating whether the employee is full-time, part-time, seasonal, etc., is critical for determining benefit entitlements.
- Failure to report the injury location accurately: If the injury did not occur on the employer’s premises, the exact location must be provided. This can impact the evaluation of the claim.
- Leaving the nature of injury code, body part affected code, or cause of injury code blank: These codes help in categorizing the injury correctly for statistical and analysis purposes. They are crucial for processing the claim.
- Not specifying if injury or illness occurred on employer’s premises: This simple yes or no question provides critical information for assessing the claim.
- Omitting physician or hospital treatment information: Information about the initial treatment received, whether at a hospital or by another healthcare provider, is important for the claim.
- Neglecting to indicate if full wages were paid for the date of injury: This affects the calculation of benefits and must be accurately reported.
These common mistakes can easily derail the workers' compensation claim process. It's important for employers to take their time, review all information carefully, and ensure that the report is completed fully and accurately. Accuracy and attention to detail can significantly smooth the path forward for workers injured on the job, facilitating a quicker resolution to their claims and a faster return to work.
- Always double-check the employer and employee information for accuracy.
- Provide a detailed account of the incident, including specific actions, objects, or substances involved.
- Ensure dates and times are accurately recorded to reflect the sequence of events correctly.
By avoiding these errors, employers can contribute to a more efficient and effective workers' compensation system, benefiting both the injured workers and the business itself by allowing for quicker claim resolutions and minimizing disputes that could delay or complicate the process.
Documents used along the form
When completing the Tennessee Department of Labor and Workforce Development Employer’s First Report of Work Injury or Illness, several additional forms and documents often accompany this submission to ensure a comprehensive approach to reporting and managing a workplace injury or illness. These forms facilitate the process, from the initial injury reporting to the final resolution of a claim, and play a crucial role in the administration of a workers' compensation claim.
- Wage Statement (Form C-42): This document details the injured employee's earnings for the 52 weeks prior to the injury, aiding in the calculation of compensation benefits.
- Employee's Choice of Physician (Form C-42): Allows the injured employee to choose a physician from a list of approved providers for their treatment.
- Notice of Denial (Form LB-0456): In case the claim is disputed or denied by the insurance carrier or employer, this form communicates the reasons for denial to the injured employee.
- Medical Waiver and Consent (Form C-31): This form grants the employer or insurance carrier authorization to obtain medical records related to the injury or illness of the employee.
- Agreement Between Employer/Employee Choice of Physician (Form C-32): Used when there is an agreement on the choice of physician for treatment of the work-related injury.
- Request for Assistance (Form LB-0489): Employed when parties involved are unable to resolve disputes independently and require intervention from the Bureau of Workers' Compensation.
- Compromise and Release Agreement (Form LB-0923): This document outlines the terms of settlement agreed upon by the employer, the insurance carrier, and the employee, effectively resolving the claim.
- Permanent Partial Disability Agreement (Form LB-1099): Used when an employee has reached maximum medical improvement and there is an agreement on the extent of the permanent disability resulting from the injury.
It is essential for employers and their insurance carriers to familiarize themselves with these documents and have a clear understanding of their purposes. Timely and accurate completion of these forms not only complies with Tennessee Workers' Compensation Law but also supports an expedited claims process, ensuring that injured employees receive the medical attention and compensation benefits they are entitled to without unnecessary delay.
Similar forms
The Workers' Compensation Claims Form, used in various states across the U.S., shares similarities with the Tennessee First Report form in terms of its primary objective. Both documents are designed to report workplace injuries or illnesses to relevant insurance carriers and authorities. They collect detailed information on the injured employee, the employer, and the specific circumstances surrounding the injury or illness, utilizing fields for employer and insurance carrier details, the nature of the business, and specifics about the injury or illness, including how and where it occurred, the body part affected, and the initial medical treatment provided.
An OSHA Injury and Illness Incident Report, as mandated by the Occupational Safety and Health Administration, has a notable resemblance to the Tennessee First Report form. It focuses on documenting occupational injuries or illnesses to ensure workplace safety and compliance with federal regulations. Both forms include detailed descriptions of the injury or illness, the time and location it occurred, personal information about the injured or ill worker, and the nature of the treatment received immediately following the incident.
The Employer’s Wage Verification Form, pertinent in workers' compensation cases, has its parallels through the inclusion of detailed employee information. While the Tennessee First Report form gathers comprehensive data about the employee's job, including their occupation, wage, employment status, and time of the work-related incident, the Wage Verification Form focuses on verifying the employee’s earnings to accurately determine compensation benefits. Both forms serve critical roles in the workers' compensation process by ensuring employees receive appropriate benefits based on accurate employment and injury details.
A Disability Benefits Claim Form, typically used to file for short-term or long-term disability benefits outside of work-related incidents, shares similar features with the Tennessee First Report in its structure and objectives. It captures comprehensive information about the claimant, including personal details, the nature of the illness or injury, and employment information. Both forms are integral in initiating the process to secure financial assistance during the claimant’s recovery period.
The Incident Report Form, commonly utilized within organizations to internally document any accidents or incidents, mirrors the data collection aspect of the Tennessee First Report form. It encompasses details such as the incident description, the individuals involved, and the immediate actions taken following the incident. This documentation aids in the internal management of health and safety risks and correlates to the Tennessee form's role in the external management of work-related injuries or illnesses through workers' compensation claims.
The Return to Work Form, a crucial component in managing an employee’s reintegration after a workplace injury, intersects with the Tennessee First Report by outlining the specifics of the injury and the affected employee's capacity to return to work. The Return to Work Form typically follows the reporting and treatment process initiated by documents like the Tennessee First Report, focusing on the assessment of the employee’s work abilities and any necessary accommodations or restrictions.
The Health Insurance Claim Form, used for filing medical claims with health insurance companies, shares the emphasis on detailed healthcare and patient information similar to the Tennessee First Report form. Though one pertains to general health care and the other to workers’ compensation, both require specific details about the medical services provided, the diagnosis, and the provider's information to ensure that claims are processed accurately and efficiently.
The Workplace Safety Inspection Form plays a preventative role in identifying potential hazards that could lead to injuries or illnesses similar to those reported on the Tennessee First Report form. While it functions proactively rather than reactively, it collects data on workplace conditions, safety protocols, and compliance with regulations, aiming to mitigate the risks documented in incident and injury reports.
Automobile Accident Report Forms, required for documenting vehicle incidents, share the element of capturing event specifics with the Tennessee First Report. Although one deals with on-the-job injuries and the other with vehicle accidents, both require comprehensive details about the incident, including date, time, location, parties involved, and a narrative description of how the incident occurred, to process claims and determine liability.
The General Liability Claim Form, relevant for incidents involving property damage or bodily injury where a business or entity may be held liable, parallels the thorough collection of incident-related details seen in the Tennessee First Report. Both forms are foundational in initiating a claims process, necessitating explicit information on the incident, the affected individuals, and the immediate response to effectively manage and resolve claims.
Dos and Don'ts
When filling out the Tennessee First Report form, it is essential to keep the following dos and don'ts in mind to ensure accuracy and compliance:
Do:- Provide complete and accurate information: Ensure all sections of the form are filled out with current and precise details to avoid delays or issues with the claim.
- Double-check the information for correctness: Before submission, review all entries to correct any mistakes or incomplete fields, ensuring the information matches the records.
- Include clear descriptions of the incident: When describing the injury or illness, include detailed information about what the employee was doing, how the injury occurred, and the specific body part affected.
- Report the injury promptly: Submit the form to your insurance carrier immediately after notice of the injury to comply with Tennessee Workers' Compensation Law requirements.
- Leave sections blank: Avoid leaving any part of the form incomplete. If a section does not apply, mark it as "N/A" (not applicable) instead of leaving it empty.
- Provide false or misleading information: Knowingly submitting incorrect information is a crime and can lead to severe penalties, including imprisonment, fines, and denial of insurance benefits.
- Forget to notify the claim administrator: Ensure the claim administrator is promptly notified of the injury, as this is crucial for the claims process.
- Overlook the need for detailed incident descriptions: Do not provide vague descriptions of the incident. Specific details are necessary for a clear understanding of the injury or illness and its causes.
Misconceptions
When it comes to the Tennessee First Report of Work Injury or Illness form, it's essential to clear up some common misconceptions that employers and employees alike might have. Misunderstandings can lead to mistakes in the reporting process, potentially affecting the outcome of a worker's compensation claim. Here are eight misconceptions explained:
- All work-related incidents require filing this form immediately: While it's critical to report serious injuries as soon as possible, not every incident may require an immediate report. It's essential to assess the situation and determine the severity of the injury or illness before proceeding.
- Only the employer is responsible for ensuring the form is completed: While it's primarily the employer's duty to file the report, it's also essential for the injured employee to provide accurate information about the incident and their injuries. Collaboration is key.
- The form is complicated and requires legal assistance to complete: While it's detailed, the form is designed to be completed without legal help. Employers and employees should carefully read the instructions and provide accurate information to the best of their knowledge.
- Reporting minor injuries is unnecessary: Even minor injuries should be documented. These records can help identify patterns that might indicate the need for changes in safety protocols or training.
- Only medical professionals can complete the injury or illness description: While medical details should be accurate, the initial description of the injury or illness can be completed by the employer or employee, detailing the incident's circumstances.
- If the employee returns to work immediately, filing this report isn't necessary: Regardless of whether an employee misses work, the incident should still be reported. This ensures there is documentation in case the injury or illness leads to future complications.
- Employers need to report injuries or illnesses to the Tennessee Department of Labor and Workforce Development directly: The form is typically filed with your insurance carrier, who then manages the reporting to the necessary state departments.
- The form should only be filed if the employee seeks medical treatment: The report should be completed and filed even if the employee initially declines medical treatment. This documentation is crucial for any future claims or medical needs related to the workplace incident.
Understanding these common misconceptions can help employers and employees navigate the reporting process more effectively. Accurate and timely reporting not only complies with Tennessee's workers' compensation laws but also supports a safer workplace by ensuring appropriate measures are taken following an injury or illness.
Key takeaways
Filling out and using the Tennessee First Report of Work Injury or Illness form is critical for ensuring compliance with the Tennessee Workers' Compensation Law. It's designed to document any injuries or illnesses that occur at the workplace, initiating the process for a worker to potentially receive benefits. Here are five key takeaways about this important document:
- Timely submission is crucial: The form must be completed and submitted to the insurance carrier immediately after an employer is notified of an injury. Delay in submission could complicate the claims process and potentially impact benefits.
- Accuracy is key: Providing false, incomplete, or misleading information on the form is a criminal offense and could result in imprisonment, fines, and denial of insurance benefits. It's important to carefully document the circumstances of the injury or illness as accurately and thoroughly as possible.
- Detailed documentation is necessary: The form requires detailed information about the employee, employer, and the injury or illness itself—including how the injury occurred, the nature of the injury, and any treatment received. Accurate documentation helps ensure that the claim is processed smoothly.
- Understanding your responsibilities: Employers must familiarize themselves with the form and the information required. This includes knowing when and how to file it, as well as understanding the importance of prompt and accurate completion to support their employees' claims.
- The State offers support: If there are questions or uncertainties about filling out the form or about the claims process in general, employers and employees can seek assistance. Tennessee has a Benefit Review System, where workers' compensation specialists can provide help. The contact number is 1-800-332-2667 (TDD).
Comprehending the components and significance of the Tennessee First Report of Work Injury or Illness form is essential for employers. It not only helps in complying with state laws but also plays a vital role in the welfare of employees who might suffer work-related injuries or illnesses. Timely and accurate completion of the form ensures that employees receive the assistance they need, when they need it.
Popular PDF Forms
Tennessee New Hire - The Tennessee New Hire form is for reporting new, rehired, or returning employees as required for all employers in the state since October 1, 1997.
Qualified Income Trust Tennessee - Maintenance of a regular bank account alongside a QIT may be necessary for comprehensive management of the grantor's finances.