Fill Out a Valid Tn Death Certificate Example Form
In dealing with the important responsibility of handling a loved one’s final affairs, obtaining a certified copy of a death certificate is a fundamental step, one that the Tennessee Department of Health Office of Vital Records facilitates through its detailed application process. This application caters to individuals requiring certified copies of a death certificate, stipulating a fee of $15.00 per copy, a measure put in place to cover the search of records even if the search does not yield a result. It outlines the necessity for applicants to provide comprehensive details about the deceased, including full name, date of death, sex, age at death, and the place of death, alongside the name and location of the funeral home. Moreover, the application highlights the specific conditions under which cause of death information may be released—predominantly to direct family members like a parent, child, spouse, or an attorney or agency representing the decedent's estate or a qualifying family member. Applicants are also reminded to attach any pertinent legal documents if applicable and are informed about the identification requirements to process the application. This thorough approach not only ensures the integrity of the process but also underscores the state's commitment to upholding legal and ethical standards in the sensitive matter of death records.
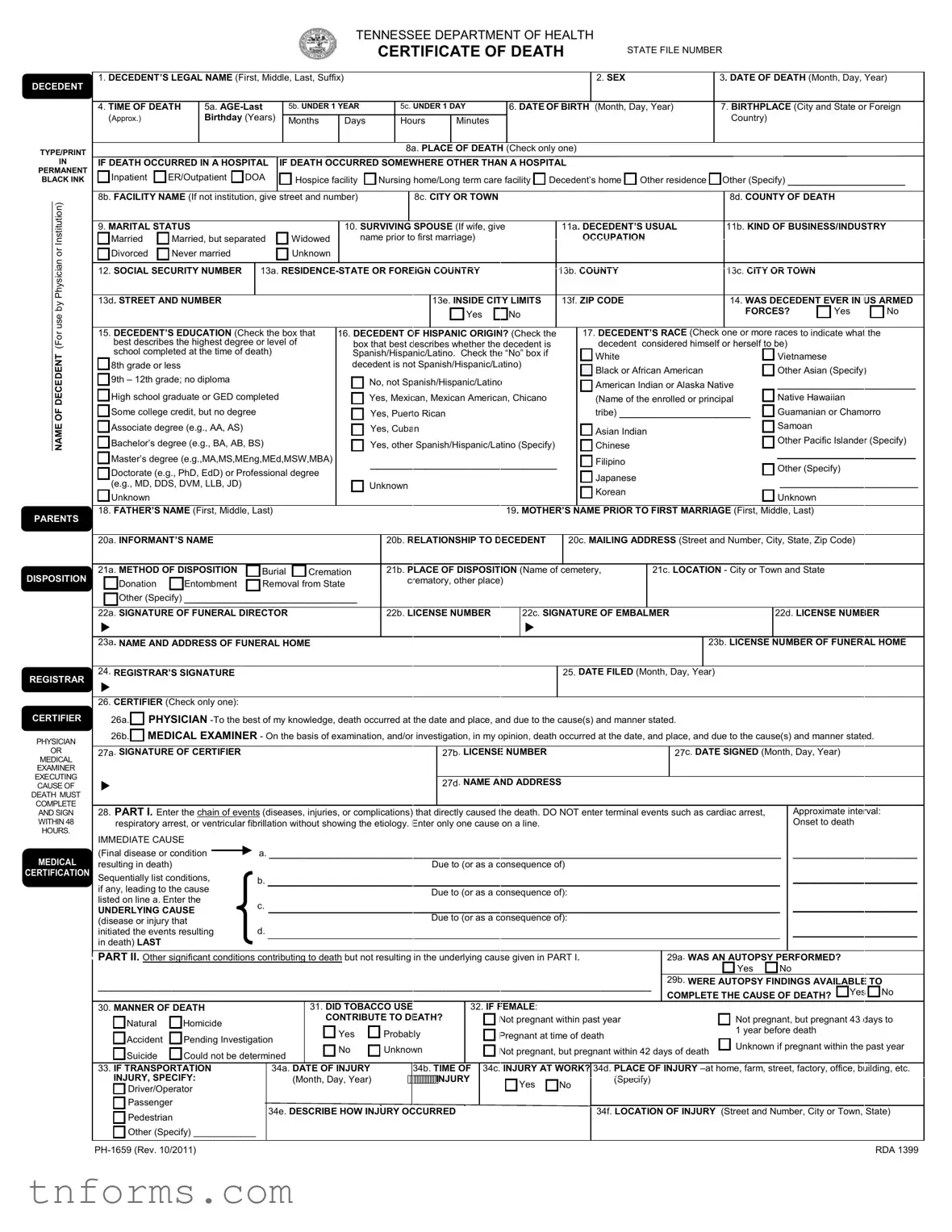
Example - Tn Death Certificate Example Form
TENNESSEE DEPARTMENT OF HEALTH
CERTIFICATE OF DEATH
STATE FILE NUMBER
DECEDENT |
1. DECEDENT’S LEGAL NAME (First, Middle, Last, Suffix) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. SEX |
|
|
|
|
|
|
3. DATE OF DEATH (Month, Day, Year) |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
4. TIME OF DEATH |
|
5a. |
|
5b. UNDER 1 YEAR |
|
|
|
5c. UNDER 1 DAY |
|
6. DATE OF BIRTH |
(Month, Day, Year) |
|
7. BIRTHPLACE (City and State or Foreign |
|||||||||||||||||||||||||||||||
|
(Approx.) |
|
|
Birthday (Years) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Country) |
|
|
|
|
|
|
|||||
|
|
|
|
Months |
Days |
|
|
|
Hours |
|
|
Minutes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE/PRINT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8a. PLACE |
OF DEATH |
(Check only one) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
IN |
IF DEATH OCCURRED IN A HOSPITAL |
IF DEATH OCCURRED SOMEWHERE OTHER THAN A HOSPITAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
PERMANENT |
|
|
|
|
|
|
|
|
Other (Specify) _________________ |
||||||||||||||||||||||||||||||||||||
BLACK INK |
Inpatient |
ER/Outpatient |
DOA |
|
Hospice facility |
|
Nursing home/Long term care facility Decedent’s home |
Other residence |
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
________________________________________________ NAMEOF DECEDENT (For use by Physician or Institution) i(F |
8b. FACILITY NAME (If not institution, give |
street and number) |
|
|
|
|
8c. CITY OR TOWN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8d. COUNTY OF DEATH |
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
9. MARITAL STATUS |
|
|
|
|
|
|
|
|
|
10. SURVIVING |
SPOUSE (If wife, give |
11a. DECEDENT’S USUAL |
|
11b. KIND OF BUSINESS/INDUSTRY |
|||||||||||||||||||||||||||||||
Married |
Married, but separated |
Widowed |
name prior to first marriage) |
|
|
|
|
|
|
OCCUPATION |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
Divorced |
Never married |
|
|
|
|
|
Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
12. SOCIAL SECURITY NUMBER |
13a. |
|
|
|
13b. COUNTY |
|
|
|
|
|
|
|
13c. CITY OR TOWN |
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
13d. STREET AND NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
13e. INSIDE CITY LIMITS |
13f. ZIP CODE |
|
|
|
|
|
|
|
14. WAS DECEDENT EVER IN US ARMED |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
FORCES? |
Yes |
No |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
15. DECEDENT’S EDUCATION (Check the box that |
16. DECEDENT OF |
HISPANIC ORIGIN? (Check the |
|
|
|
17. DECEDENT’S RACE (Check |
one or more races to indicate what the |
|
|||||||||||||||||||||||||||||||||||||
best describes the highest degree or level of |
box that best describes whether the decedent is |
|
|
|
|
decedent |
considered himself or herself to be) |
|
|
|
|||||||||||||||||||||||||||||||||||
school completed at the time of death) |
|
|
Spanish/Hispanic/Latino. Check the “No” box if |
|
|
|
|
White |
|
|
|
|
|
|
|
|
Vietnamese |
|
|
||||||||||||||||||||||||||
8th grade or less |
|
|
|
|
|
|
|
|
|
decedent is not Spanish/Hispanic/Latino) |
|
|
|
|
Black or African American |
|
|
Other Asian (Specify) |
|
||||||||||||||||||||||||||
9th – 12th grade; no diploma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
No, not Spanish/Hispanic/Latino |
|
|
|
|
American Indian or Alaska Native |
____________________ |
||||||||||||||||||||||||||||||||
High school graduate or GED completed |
|
|
Yes, Mexican, Mexican American, Chicano |
|
|
|
|
(Name of the enrolled or principal |
Native Hawaiian |
|
|
||||||||||||||||||||||||||||||||||
Some college credit, but no degree |
|
|
|
Yes, Puerto Rican |
|
|
|
|
|
|
|
tribe) ___________________ |
Guamanian or Chamorro |
|
|||||||||||||||||||||||||||||||
Associate degree (e.g., AA, AS) |
|
|
|
|
|
|
|
|
Yes, Cuban |
|
|
|
|
|
|
|
|
|
|
|
|
Asian Indian |
|
|
Samoan |
|
|
||||||||||||||||||
Bachelor’s degree (e.g., BA, AB, BS) |
|
|
|
Yes, other Spanish/Hispanic/Latino (Specify) |
|
|
|
|
Chinese |
|
|
|
|
|
|
|
|
Other Pacific Islander (Specify) |
|||||||||||||||||||||||||||
|
Master’s degree (e.g.,MA,MS,MEng,MEd,MSW,MBA) |
|
___________________________ |
|
|
|
|
Filipino |
|
|
|
|
|
|
|
|
____________________ |
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other (Specify) |
|
|
|||||||||||||||||||||||||||||
|
Doctorate (e.g., PhD, EdD) or Professional degree |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Japanese |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
____________________ |
||||||||||||||||||
|
(e.g., MD, DDS, DVM, LLB, JD) |
|
|
|
|
|
|
|
Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Korean |
|
|
|
|
|
|
|
|
|||||||||||||||||
|
Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unknown |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
PARENTS |
18. FATHER’S NAME (First, Middle, Last) |
|
|
|
|
|
|
|
|
|
|
|
|
|
19. MOTHER’S |
NAME PRIOR TO FIRST MARRIAGE (First, Middle, Last) |
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
20a. INFORMANT’S NAME |
|
|
|
|
|
|
|
|
|
|
20b. RELATIONSHIP TO |
DECEDENT |
|
20c. MAILING ADDRESS (Street and Number, City, State, Zip Code) |
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
DISPOSITION |
21a. METHOD OF DISPOSITION |
|
Burial |
|
Cremation |
|
|
21b. PLACE OF DISPOSITION (Name of |
cemetery, |
|
21c. LOCATION - City or Town and State |
|
|
||||||||||||||||||||||||||||||||
Donation |
Entombment |
|
Removal from State |
|
|
|
crematory, other place) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
Other (Specify) _________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
22a. SIGNATURE OF FUNERAL DIRECTOR |
|
|
|
|
|
22b. LICENSE NUMBER |
|
|
22c. SIGNATURE OF EMBALMER |
|
|
22d. LICENSE NUMBER |
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
23a. NAME AND ADDRESS OF FUNERAL HOME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
23b. LICENSE |
NUMBER OF FUNERAL HOME |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
REGISTRAR |
24. REGISTRAR’S SIGNATURE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
25. DATE FILED (Month, Day, Year) |
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
26. CERTIFIER (Check only one): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
CERTIFIER |
26a. PHYSICIAN |
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
PHYSICIAN |
26b. MEDICAL EXAMINER - On the basis of examination, and/or investigation, in my opinion, death occurred at the date, and place, and due to the cause(s) and manner stated. |
|
|||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OR |
27a. SIGNATURE OF CERTIFIER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
27b. LICENSE NUMBER |
|
|
|
|
|
|
|
|
27c. DATE SIGNED (Month, Day, Year) |
|
|
||||||||||||||||||
MEDICAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EXAMINER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EXECUTING |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
27d. NAME AND ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
CAUSE OF |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
DEATH MUST |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMPLETE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AND SIGN |
28. PART I. Enter the chain of events (diseases, injuries, or complications) that directly caused the death. DO NOT enter terminal events such as cardiac arrest, |
|
|
|
Approximate interval: |
|
|||||||||||||||||||||||||||||||||||||||
WITHIN 48 |
respiratory arrest, or ventricular fibrillation without showing the etiology. Enter only one cause on a line. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Onset to death |
|
||||||||||||||||||||||||||
HOURS. |
IMMEDIATE CAUSE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
a. __________________________________________________________________________ |
|
__________________ |
|||||||||||||||||||||||||||||||||||||||
MEDICAL |
(Final disease or condition |
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|||||||||||||||||||||||||||||||||||||||||||
resulting in death) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Due to (or as a consequence of) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
CERTIFICATION |
Sequentially list conditions, |
|
b. __________________________________________________________________________ |
|
__________________ |
||||||||||||||||||||||||||||||||||||||||
|
if any, leading to the cause |
|
|
|
|
|
|
|
|
|
|
|
|
|
Due to (or as a consequence of): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
listed on line a. Enter the |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
__________________ |
|||||||||||||||
|
|
|
|
c. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
UNDERLYING CAUSE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
(disease or injury that |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Due to (or as a consequence of): |
|
|
|
|
|
|
|
|
|
|
|
|
|
__________________ |
||||||||||||||
|
initiated the events resulting |
|
d. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
MEDICAL |
in death) LAST |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CERTIFICATION |
PART II. Other significant conditions contributing to death but not resulting in the underlying cause given in PART I. |
|
|
|
|
29a. WAS AN AUTOPSY |
PERFORMED? |
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
|
||
|
________________________________________________________________________________ |
29b. WERE AUTOPSY FINDINGS AVAILABLE TO |
|||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMPLETE THE CAUSE OF DEATH? |
Yes |
No |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
30. MANNER OF DEATH |
|
|
|
|
|
|
31. DID TOBACCO USE |
|
|
|
32. IF FEMALE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
Natural |
Homicide |
|
|
|
|
|
|
CONTRIBUTE TO DEATH? |
|
|
Not pregnant within past year |
|
|
|
|
|
|
|
Not pregnant, but pregnant 43 days to |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
Yes |
|
|
Probably |
|
|
|
|
|
Pregnant at time of death |
|
|
|
|
|
|
|
1 year before death |
|
|
||||||||||||||||||
|
Accident |
Pending Investigation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unknown if pregnant within the past year |
||||||||||||||||||||||||||||
|
|
|
No |
|
|
Unknown |
|
|
|
|
|
Not pregnant, but pregnant within 42 days of death |
|
||||||||||||||||||||||||||||||||
|
Suicide |
Could not be determined |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
33. IF TRANSPORTATION |
|
|
34a. DATE OF INJURY |
|
|
|
|
34b. TIME OF |
34c. INJURY AT WORK? |
34d. PLACE OF INJURY |
||||||||||||||||||||||||||||||||||
|
INJURY, SPECIFY: |
|
|
|
|
|
|
|
(Month, Day, Year) |
|
|
|
INJURY |
|
|
Yes |
No |
|
(Specify) |
|
|
|
|
|
|
|
|
||||||||||||||||||
|
Driver/Operator |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Passenger |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
34e. |
DESCRIBE HOW INJURY OCCURRED |
|
|
|
|
|
|
|
34f. LOCATION OF INJURY (Street and Number, City or Town, State) |
|||||||||||||||||||||||||||||||
|
Pedestrian |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Other (Specify) ____________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RDA 1399 |
||||
Form Breakdown
| Fact | Detail |
|---|---|
| Application Submission Department | Tennessee Department of Health Office of Vital Records |
| Form Type | Application for Certified Copy of Certificate of Death |
| Application Fee | $15.00 per copy |
| Required Information | Full Name of Deceased, Date of Death, Sex, Age at Death, Place of Death, Name and Location of Funeral Home, Applicant's Signature, Relationship to Deceased, Purpose of Copy |
| Cause of Death Disclosure | Available only to the decedent's parent, child, spouse, or an attorney or agency acting on behalf of the decedent's estate or qualified family member. |
| Identification Requirement | Government Issued ID With Signature (or notarization of application) |
| Payment Method | Check or Money Order payable to Tennessee Vital Records |
| Record Search Scope | If no record is found, a search for the year before and the year after the provided date of death is included in the fee. |
| Contact Information for Follow-Up | If no response within 45 days, contact Tennessee Vital Records at 615-741-1763. |
Detailed Instructions for Filling Out Tn Death Certificate Example
Obtaining a certified copy of a death certificate is a necessary step for a variety of reasons, including settling estates, accessing benefits, and handling personal affairs of the deceased. The process requires careful attention to detail to ensure accuracy and compliance with state requirements.
- Start by indicating the Date of application at the top of the Tennessee Department of Health Office of Vital Records form.
- Enter the Number of Copies you wish to receive in the space provided.
- Enclose the appropriate fee with your application, noting that the form specifies a charge of $15.00 for each copy requested.
- Write the Full Name of the Deceased, including First, Middle, and Last Name.
- Fill in the Date of Death, specifying the Month, Day, and Year.
- Indicate the deceased's Sex by checking either Male or Female.
- Enter the Age at Death.
- Provide the Place of Death, including City, County, and State.
- List the Name of the Funeral Home and the Location of the funeral home, again including City, County, and State.
- Sign the form under Signature of Person Making Request.
- Specify your Relationship to the Deceased.
- Indicate the Purpose of Copy.
- If applicable, check YES or NO for whether you want the certificate to show the Cause of Death. Remember, this information is available only to specific family members or legal representatives.
- Provide a Telephone Number where you can be reached for additional information.
- Ensure a Government Issued ID is included with your signature, as required to verify your identity.
- Print the name and address of the person to whom the certified copy is to be mailed in the "FILL OUT BELOW/ DO NOT DETACH" section. This includes Name, Address or Route, City, State, and Zip Code.
- Send the completed application along with your check or money order and a photocopy of your government-issued ID to: Tennessee Vital Records Andrew Johnson Tower, 1st Floor, 710 James Robertson Parkway, Nashville, TN 37243.
After the application is submitted, if no response is received within 45 days, it's recommended to follow up by writing or calling Tennessee Vital Records directly. The careful completion of each step ensures a smooth process in obtaining the necessary document during what can be a challenging time.
More About Tn Death Certificate Example
What is the process for obtaining a certified copy of a death certificate in Tennessee?
To obtain a certified copy of a death certificate in Tennessee, an individual must complete the Application for Certified Copy of Certificate of Death form. This form requires the full name of the deceased, date of death, place of death, and the requester's relationship to the deceased among other details. A fee of $15.00 per copy must accompany the application. The completed application, along with the required fee and a photocopy of a government-issued ID of the requester, should be mailed to Tennessee Vital Records at the specified address. If the death certificate can't be located with the provided information, a search for the year before and after the provided date of death will be conducted without additional charges.
Who can request a certified copy of a death certificate in Tennessee?
In Tennessee, a certified copy of a death certificate can be requested by the decedent's parent, child, spouse, or an attorney or agency acting on behalf of the decedent's estate or a qualifying family member. Copies of any legal documents may be required to establish the relationship or authority of the requester in relation to the deceased.
How much does it cost to obtain a certified copy of a death certificate in Tennessee?
The fee for obtaining a certified copy of a death certificate in Tennessee is $15.00. This fee includes the search for the records, even if no record is found, and covers one certified copy of the death certificate if the record is located. Additional copies would require an additional fee of $15.00 each.
Is it possible to get the cause of death on the death certificate?
Yes, it is possible to have the cause of death included on the death certificate, but this information is only available to the decedent's parent, child, spouse, or an attorney or agency acting on behalf of the decedent's estate or a qualifying family member. A requestor must indicate on the application if they want the death certificate to show the cause of death.
What identification is needed to request a death certificate?
When requesting a certified copy of a death certificate in Tennessee, the requester must provide a photocopy of a government-issued ID that includes their signature. This requirement ensures the protection of personal information and complies with state law.
What happens if the death certificate cannot be found?
If the requested death certificate cannot be found with the initial details provided, Tennessee Vital Records will conduct an additional search for records from the year before and the year after the indicated date of death. This expanded search is included in the $15.00 fee and helps ensure all efforts are made to locate the certificate.
How long does it take to receive a certified copy of a death certificate in Tennessee?
Applicants should expect to receive a response or the requested certified copy of a death certificate within 45 days from the date Tennessee Vital Records receives the application. If no response has been received within this timeframe, it is recommended to contact Tennessee Vital Records directly for an update.
Common mistakes
Filling out official documents can sometimes be daunting. When it comes to the Tennessee Death Certificate Example form, it's important to approach it with attention to detail to ensure all information is accurately captured. However, several common mistakes can occur during this process. By identifying these, individuals can avoid unnecessary delays or issues in obtaining a certified copy of a death certificate.
- Incorrectly listing the full name of the deceased: It's crucial to ensure the deceased's first, middle, and last names are correctly spelled and placed in the appropriate fields. Any discrepancy can lead to confusion or misfiled records.
- Forgetting to include the application fee: A common oversight is neglecting to enclose the $15.00 fee per copy requested. This omission can halt the process until the fee is received.
- Misstating the number of copies needed: Often, individuals underestimate the number of certified copies required for different legal and personal purposes. It's advisable to carefully consider and correctly state the needed quantity.
- Incorrect date of death: Filling in the wrong date can significantly delay the search process, as the records may not be found under the incorrect information provided.
- Leaving the sex and age at death fields blank: These details are pivotal for proper identification and must be accurately filled to avoid processing delays.
- Not specifying the relationship to the deceased: This is essential information that confirms eligibility to receive the death certificate. Failing to provide it can lead to a request being denied.
- Forgetting to check the cause of death box: If you're eligible and wish to have the cause of death included, it's important not to overlook this option.
- Lacking ID or notarization: Failing to include a photocopy of a government-issued ID or to have the application notarized (if the ID is not provided) can make it impossible to process the request.
While these mistakes are common, they are also avoidable. Taking the time to carefully review and accurately fill out the Tennessee Department of Health's death certificate application form can streamline the process. Remember, details matter in these instances, not only for legal clarity but also as a respectable record of a person's passing.
- Ensure all names and dates are double-checked for accuracy.
- Include the correct fee and consider the needed number of copies.
- Don't overlook any field, especially those that specify relationships and request for cause of death information.
By avoiding these common errors, individuals can facilitate a smoother transaction with the Tennessee Department of Health Office of Vital Records. This not only honors the deceased by efficiently handling their final documents but also eases the process for those grieving, during a time when even small tasks can feel overwhelming.
Documents used along the form
When an individual passes away, the process of handling their affairs often necessitates more than just obtaining a certified copy of a death certificate. Several documents and forms commonly accompany the Tennessee Department of Health Office of Vital Records Application for Certified Copy of Certificate of Death to efficiently manage the deceased's estate, insurance, and other related matters. These documents are essential for legal, financial, and personal reasons, providing necessary proof and authority to carry out various tasks and requests.
- Will: A legal document that outlines the deceased’s wishes regarding the distribution of their estate and care for any minor children.
- Letters of Administration or Letters Testamentary: These are issued by a court to appoint someone to manage the deceased's estate according to the will or, if there's no will, according to state laws.
- Trust Documents: If the deceased established any trusts, these documents would need to accompany the death certificate to manage or distribute the trusts according to the deceased's wishes.
- Life Insurance Forms: To claim life insurance benefits, the insurer will require a death certificate and possibly additional forms filled out by the beneficiary.
- Bank Forms: Banks often require a certified death certificate to close accounts, access safety deposit boxes, or transfer ownership of accounts.
- Pension/Retirement Account Forms: To claim or manage the deceased's pension or retirement accounts, the administrating organizations will require a death certificate and beneficiary forms.
- Property Titles and Deeds: To transfer ownership of property, titles, and deeds will need to be reissued, requiring a copy of the death certificate.
- Vehicle Titles and Registration Documents: Similar to property titles, transferring a vehicle's title and registration requires a death certificate.
- Affidavit of Heirship: In the absence of a will, this document helps establish the legal heirs of the deceased for distribution of property according to state law.
- Funeral Home Contracts and Documents: These outline the arrangements and financial transactions made with the funeral home, often needed for reimbursement from estate funds or life insurance.
Together with the Tennessee Death Certificate, these documents serve a crucial role in settling the affairs of the deceased. Obtaining, completing, and filing these documents promptly and correctly can significantly ease the administrative burden on the deceased’s loved ones, allowing them to focus on grieving and healing. It is advisable to consult with a legal professional to ensure that all necessary paperwork is handled correctly and in accordance with the law.
Similar forms
Birth certificates are documents that have notable similarities to death certificates, such as the Tennessee Certificate of Death. Both serve as official records managed by state departments of health or vital records. While a birth certificate marks the entry of an individual into the world, providing details such as name, date of birth, parentage, and birthplace; a death certificate records the departure, including the deceased's full name, date and place of death, and often cause of death. Each document is crucial for legal, personal, and public health purposes, serving to establish identity, familial relationships, and demographic statistics.
Marriage licenses are another category of vital records akin to death certificates. Similar to how a death certificate outlines the end of a person's life, a marriage license documents the legal union between two individuals. Details commonly found on these documents include full names, dates of birth, places of marriage, and the officiating authority. Although serving different life events, both types of documents are integral for legal processes, such as inheritance rights, insurance claims, and changing one's name or marital status.
Divorce decrees, while marking the dissolution of a legal union as opposed to the end of life, share critical functionalities with death certificates. These documents bear legal significance in evidencing the termination of a marital relationship, providing specifics such as the names of the parties, the date of the divorce, and terms of the settlement. Like death certificates, divorce decrees are essential for various legal transactions including property settlements, name changes, and remarriage permissions.
Adoption records are significant legal documents that, while marking a joyous occasion of expanding a family, share some procedural and legal commonalities with death certificates. For instance, adoption records formalize the creation of a parent-child relationship, detailing names of adoptive parents, the child's name (which may be legally changed through the adoption), and the date the adoption took place. Both documents require official processes through legal authorities to record and acknowledge significant life changes.
Court orders can have specific similarities to death certificates in their legal authority to document and mandate significant changes or statuses for individuals. For instance, a court order can determine the guardianship of a minor, the allocation of a deceased person’s estate, or mandate changes to legal documents. Like death certificates, they serve as indisputable proof of legal actions and decisions, impacting various aspects of personal, legal, and civil matters.
Last wills and testaments, though not directly akin to a standardized form like a death certificate, intersect with the procedures following an individual’s death. They specify a deceased person's wishes regarding the distribution of their estate and care of minor children, among other directives. The execution of a will often requires referencing the death certificate to ascertain the passing of the individual in question, underlining the death certificate’s role in the facilitation of posthumous wishes.
Passports, while primarily identified as travel documents, also possess attributes similar to those of death certificates in terms of identity verification. Just as a death certificate provides undisputable evidence of an individual's death, a passport confirms a person's nationality and identity to governmental and international authorities. Both are official documents issued by government bodies, and each plays a pivotal role in personal identification and the execution of certain legal rights and privileges.
Dos and Don'ts
When you're filling out the Tennessee Death Certificate Example form, it can seem straightforward, but details matter a lot. Here are some do's and don'ts that can help ensure the process goes smoothly and accurately.
Do:- Write legibly: Make sure that every word on the application is readable. This helps avoid errors or delays in processing.
- Include accurate information: Double-check all details you enter against official documents to ensure accuracy.
- Use a black ink pen: This makes the application easier to read and photocopy, if necessary.
- Provide a government-issued ID: A photocopy of a government-issued ID with your signature is required unless the application is notarized.
- Verify the fee: Confirm that the fee is still $15.00 per copy as this could change. Always check the latest requirements on the Tennessee Department of Health website.
- Include all necessary documents: If you're requesting the cause of death, ensure you're entitled to this information and submit any required legal documents.
- Send cash: For your own security and to follow the application instructions, send a check or money order.
- Guess on details: If you're unsure about any information, such as the exact date of death, verify it with another source before submitting.
- Leave fields blank: If a section does not apply, write 'N/A'. This indicates that you didn't just forget to fill it out.
- Rush through the form: Take your time to understand each request and provide thoughtful, accurate responses.
- Forget to sign: Your signature is necessary to process the application. Make sure you sign the form where indicated.
- Ignore the notarization option: If your application is notarized, you may not need to include a photocopy of your ID. Consider this for faster processing.
Misconceptions
When it comes to obtaining a death certificate in Tennessee, there are several misconceptions that can create confusion. Understanding these misconceptions can help streamline the process and set appropriate expectations. Here are ten common misconceptions about the Tennessee Death Certificate Example form:
- Anybody can request a death certificate. In reality, cause of death is only available to the decedent's immediate family members, attorneys, or agencies acting on behalf of the decedent's estate or qualifying family member.
- Online applications are available for everyone. While information can be found online, submitting a notarized application or providing a government-issued ID is necessary to process the request.
- Death certificates are free. There is a $15.00 fee for each copy requested, which covers the search of the records even if the record is not found.
- Cash payments are accepted through mail. The application specifically advises not to send cash. Payments should be made via check or money order.
- You will get your certificate immediately. If there is no response within 45 days, you are encouraged to contact Tennessee Vital Records. This implies that obtaining a certificate can take an extended amount of time.
- Death certificates show cause of death for everyone. The option to show the cause of death on the certificate is only available to certain requesters due to privacy concerns.
- It's illegal to request a death certificate for genealogy purposes. While the form asks for the purpose of the copy, it doesn't specifically forbid genealogy. However, access to the cause of death might be restricted.
- Any discrepancies or errors on a death certificate are permanent. While the form doesn’t discuss correction processes, in general, vital records offices have procedures for amending records.
- You need to know the exact date of death to request a certificate. If the exact date of death provided does not find a record, the search will include the year before and after the date provided within the fee.
- Only Tennessee residents can request a death certificate from the Tennessee Department of Health Office of Vital Records. The form does not state any residency requirement, implying that non-residents can also request a death certificate as long as they can provide the necessary documentation and fee.
Understanding these misconceptions can make the process of obtaining a death certificate in Tennessee more straightforward, helping individuals get the vital records they need in a timely manner.
Key takeaways
Requesting a death certificate is a process that takes serious attention to detail and understanding of the necessary steps. Here are five key takeaways for those filling out and using the Tennessee Death Certificate Example form:
- Accuracy is crucial when providing information. Everything from the full name of the deceased to the place of death must be accurately entered to ensure the request can be processed smoothly.
- A fee of $15.00 per copy is required with the application. This fee covers the search of records even if no record is found. It is advisable to provide the exact amount in the form of a check or money order, as cash is not accepted.
- The form makes it clear that access to the cause of death is limited to specific individuals such as the parent, child, spouse of the deceased, or an attorney acting on behalf of the deceased’s estate or qualifying family member. This restriction underscores the need for confidentiality and the protection of sensitive information.
- Applicants must send a photocopy of a government-issued ID along with the application if it is not notarized. This step is important for verifying the identity of the person making the request and preventing potential misuse of the information.
- If a response has not been received within 45 days, the applicant is encouraged to follow up by writing or calling Tennessee Vital Records. This implies the importance of keeping records of the application and monitoring its progress, ensuring that the request is being processed.
Following these guidelines will help streamline the process, making it easier for family members to access vital records in a time of need. Understanding the requirements and preparing accordingly will save time and reduce the stress associated with obtaining these important documents.
Popular PDF Forms
How Long Does It Take for a Divorce to Be Final in Tennessee - This comprehensive form serves as the final decree in a Tennessee divorce, outlining the legal termination of marriage and associated agreements.
Tennessee Cc 3 - The document’s revision history indicates its evolution to address the administrative needs of the DBE program effectively.
Class D License Tn - This form is utilized by the Tennessee Department of Safety and Homeland Security for drivers to report accidents.